Polynucleotides and PDRN: the new generation of regenerative skin boosters
Injectable cosmetology is gradually shifting its focus from simply filling volume and providing hydration toward deep skin regeneration. While not long ago the main request was to "remove a wrinkle" or "add radiance," today more and more practitioners work at the level of cellular repair. At the center of this direction are polynucleotides (PN) and polydeoxyribonucleotides (PDRN) – products that don't mask age-related changes but instead trigger the dermis's own restorative processes.
What polynucleotides and PDRN are
To understand how they work, it's worth going back to basic biochemistry. Nucleotides are organic molecules made up of sugar, phosphate, and a nitrogenous base. When they link into long chains, they form polynucleotides – the very structures that DNA and RNA are built from.
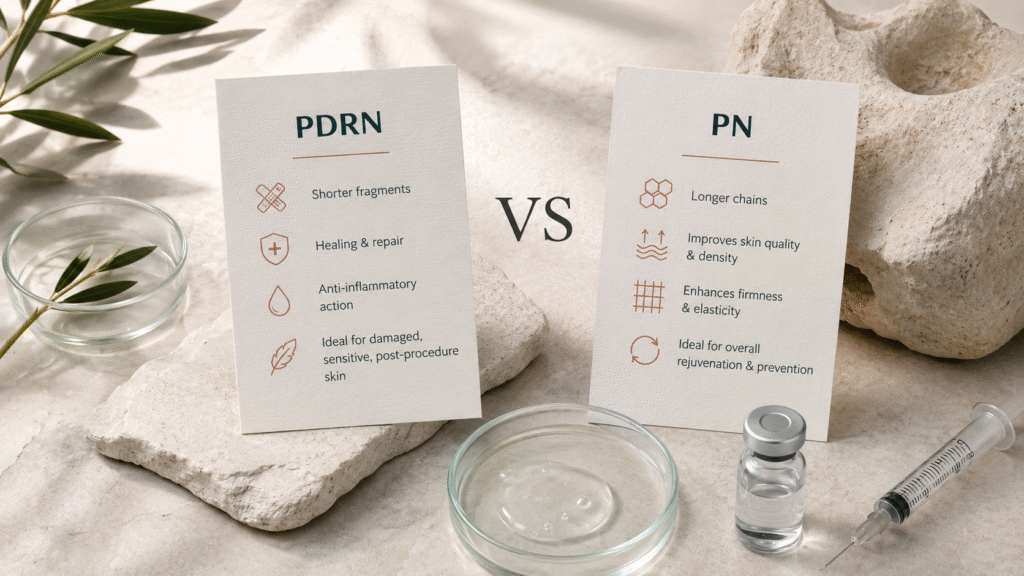
In aesthetic medicine, purified fragments of nucleotide chains are used, having gone through a high degree of filtration and sterilization. PDRN consists of shorter fragments with a pronounced restorative and anti-inflammatory action, whereas polynucleotides are longer chains and work primarily on the overall quality and density of the skin. Both classes of products are biocompatible, gradually break down within the tissues, and don't create foreign volume.
Mechanism of action
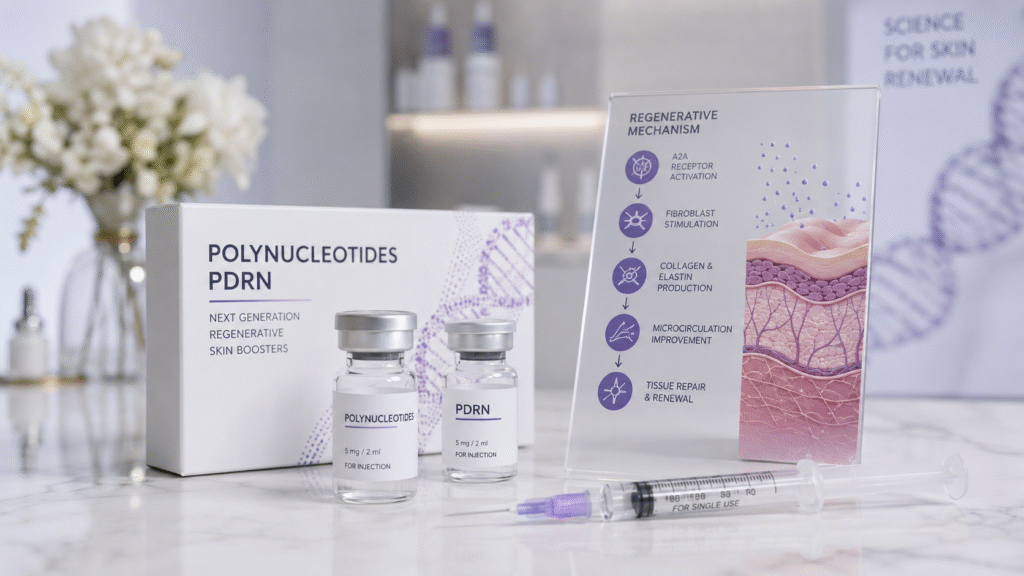
The key feature of regenerative boosters is biostimulation rather than filling. The active fragments act on adenosine A2A receptors, which triggers a cascade of restorative reactions. As a result, fibroblasts are activated – the cells responsible for producing collagen and elastin.
At the same time, the products improve microcirculation, reduce oxidative stress, and decrease the inflammatory response in the tissues. In addition, the nucleotide fragments serve as building material for the skin's own cells, as they break down, they release components that the tissues use in repair processes. This explains why regenerative boosters are especially effective wherever the skin is weakened or damaged.
The skin receives not a temporary cosmetic effect but a stimulus for self-renewal. That's precisely why the result develops gradually and lasts longer than with classic hydration using hyaluronic acid. In essence, the practitioner doesn't introduce a finished result from the outside but creates the conditions in which the tissue restores itself.
PN and PDRN: what's the difference
Despite their close origin, the two classes of products address slightly different tasks. PDRN is geared toward healing and repair, it's especially effective for damaged, sensitive skin, post-acne, after aggressive procedures, and in cases of pronounced tissue reactivity. Polynucleotides with longer chains work on the overall quality of the skin – increasing density and firmness, smoothing fine lines, and improving tone.
In practice, the practitioner chooses the product based on the priority. If the goal is to restore and calm the skin, an emphasis on PDRN makes sense. If the goal is comprehensive rejuvenation and the prevention of age-related changes, polynucleotide complexes are more often chosen.
How they differ from fillers and conventional skin boosters
It's important not to confuse regenerative boosters with hyaluronic acid fillers. Fillers based on cross-linked hyaluronic acid create volume and correct contours – they're a structural tool. Classic skin boosters with non-cross-linked hyaluronic acid provide deep hydration but act primarily as a reservoir of moisture.
Polynucleotides and PDRN differ fundamentally, they don't add volume and don't work as a simple moisturizer but rather rebuild the tissue itself from within by stimulating cellular activity. That's why they're often called bioremodelers or regenerative boosters. This is a different level of action – directed not at the symptom but at the cause of declining skin quality.
Indications
Regenerative boosters are indicated for a wide range of aesthetic tasks. These include reduced skin firmness and tone without pronounced volume loss, a dull complexion, dehydration, fine superficial wrinkles, and uneven texture. The products are effective for thinned and sensitive skin, for post-acne marks, and as preparation for more invasive procedures or recovery after them.
A separate direction is prevention. In younger patients, regenerative boosters are used to maintain skin quality and slow the first signs of aging. Treatment areas include the face, neck, décolletage, hands, and the periorbital region, where the skin is especially thin and requires a delicate approach.
Protocols and treatment course
Since the effect is cumulative in nature, regenerative boosters are applied as a course. The standard scheme is from two to four sessions with an interval of two to four weeks. Maintenance sessions are usually performed once every few months.
Patients notice the first changes after one to two weeks, the skin becomes more hydrated and fresh. The maximum result unfolds four to six weeks after the course is completed, when the synthesis of new collagen is activated. The product is injected with fine needles into the superficial and middle layers of the dermis – the technique can be either linear-retrograde or papular, depending on the product and the area.
Combining with other methods
Regenerative boosters combine well with most aesthetic procedures. A common protocol is the combination with microdosed administration of botulinum toxin, the booster improves skin quality, while the toxin corrects muscle activity, which together produces a natural rejuvenating effect.
The products are also combined with fillers when it's necessary to restore both volume and tissue quality at the same time, and with device-based methods – fractional laser rejuvenation, microneedling, and radiofrequency therapy. In such protocols, regenerative boosters speed up recovery and enhance the overall result. When building a combined scheme, it's important to observe the intervals and the sequence of procedures.
Contraindications and precautions
Like any injectable procedure, the administration of polynucleotides and PDRN has limitations. These include pregnancy and the lactation period, acute infectious and inflammatory processes, blood-clotting disorders, autoimmune diseases in the acute stage, and individual intolerance to the components. Inflammation or damage to the skin in the area of the intended injection also calls for postponing the procedure.
Seven to ten days before the session, it's recommended to discontinue medications that affect blood clotting. After the procedure, during the first 24 hours, it's worth avoiding intense physical activity, sauna visits, and facial massage.
What the practitioner should keep in mind
The result depends directly on the practitioner's qualifications and the quality of the product. A consultation is necessary before the procedure, with an assessment of the skin's condition and an analysis of its type and individual characteristics. The competent selection of a product – PDRN, polynucleotides, or a combination of them – is already half the success.
Just as important are the authenticity of the product and compliance with storage and transport conditions. Regenerative boosters are sensitive to the temperature regime, so it's worth working only with verified products from reliable suppliers with a complete package of accompanying documents.
Common misconceptions
A number of persistent myths have built up around regenerative boosters. The first is that they deliver an instant visible result, like fillers. In reality, the effect is cumulative, and it's important to prepare the patient in advance for a course-based approach. The second myth is that a single procedure is enough, without a full course, the product's potential is only partially realized. The third is the idea that regenerative boosters can replace fillers in cases of pronounced volume loss. That's not the case: they improve tissue quality but don't create structural volume, which is why for serious contouring tasks they're combined with fillers rather than set against them.
Polynucleotides and PDRN reflect the main trend of modern aesthetic medicine – the shift from correction to regeneration. These products don't mask age-related changes but instead restore the skin's capacity for self-repair, improving its density, firmness, and overall quality. For the practitioner, this is a flexible tool that can be used both on its own and as part of comprehensive protocols, expanding the range of services and offering patients a natural and long-lasting result.